What is the relationship between vitamin B12 deficiency and tongue health?
This connection is quite significant.
Have you ever come across the terms “B12 deficiency tongue” or “pernicious anemia tongue”? What people describe is glossitis. It happens when the enlarged red blood cells that often accompany B12 deficiency result in inflammation and depapillation of the dorsal surface of the tongue, leaving it beefy, fiery-red, and sometimes sore. Additionally, it can make the tongue appear smooth due to swelling. Example case:
A classic smooth, beefy red “B12 deficiency anemia tongue”
In fact, even though B12 deficiency can make the tongue sore and beefy-red, it’s not the only disease that can alter the tongue’s color, texture, and size. In other words, while B12 and tongue status are tightly related, other illnesses shouldn’t be ruled out. In addition to B12 deficiency, glossitis can be an indicator of various underlying causes, like vitamin deficiencies such as folic acid and niacin, infections, malignancies, or nerve damage.
Nonetheless, our main focus lies in the relationship between B12 and tongue health.
The Vitamin B12 Tongue
B12 deficiency impacts cell reproduction, affecting the tongue’s epithelial cells. As a result, glossitis occurs in up to 25% of cases. This illness typically manifests as a diffuse and clinically nonspecific atrophy of lingual papillae, impacting most of the tongue. It is commonly referred to as Hunter’s glossitis or Moeller-Hunter glossitis.
Vitamin B12 Deficiency Tongue Symptoms
Beefy-red or fiery-red color
Swelling
Smooth texture
Soreness
Presence of ulcers
These are the common “vitamin B12 tongue” symptoms. The soreness may result from a coexisting condition known as glossodynia or burning mouth disorder (BMD):
A 73-year-old woman presented with several months of glossodynia having previously been diagnosed by her primary care physician with primary BMD. Subsequently, she consulted an otolaryngologist, who pursued further diagnostic evaluation.
Examination revealed the presence of a beefy, red, smooth tongue, and further laboratory evaluation yielded a low serum vitamin B12 level and macrocytosis. Three months of oral vitamin B12 supplementation led to partial restoration of serum vitamin B12 levels and a modest improvement in symptoms. Her final diagnoses were atrophic glossitis and glossodynia secondary to vitamin B12 deficiency, most likely due to pernicious anemia.
The results of this case have important clinical implications for the diagnostic evaluation and management of patients with glossodynia and apparent BMD.
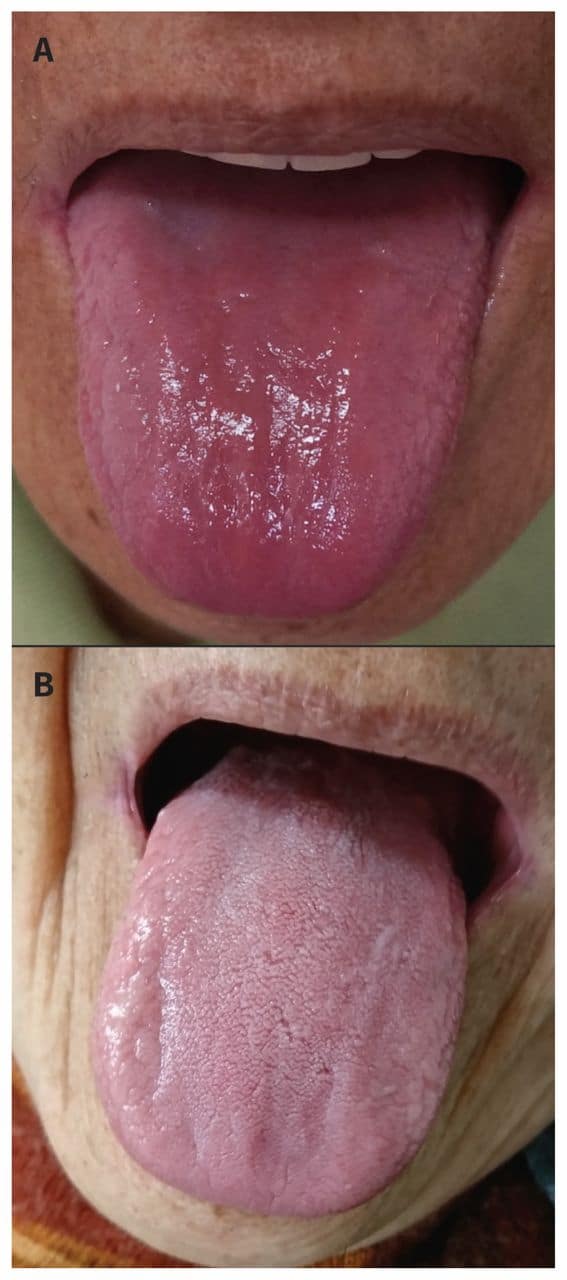
A 69-year-old Japanese woman presented with a 4-week history of painful tongue and reduced sense of taste. On physical examination, she had a smooth, red tongue without dorsal papillae, suggestive of glossitis. Results from laboratory tests were consistent with macrocytosis without anemia: mean corpuscular volume 104.9 (normal range 80–97) fL, hemoglobin 121 (normal range 110–165) mmol/L, iron 10.92 (normal range 8.95–26.85) μmol/L, ferritin 72 (normal range 5–157) μg/L and serum vitamin B12 77.49 (normal range 147.6–442.8) pmol/L. In addition, an endoscopic biopsy of her gastric mucosa showed atrophic gastritis, and the result from a test for the presence of serum anti-intrinsic antibodies was positive. We diagnosed pernicious anemia.
We prescribed intramuscular methylcobalamin for our patient’s pernicious anemia, and her painful tongue and reduced sense of taste resolved within days. Her tongue regained its normal appearance within a month. She remains on maintenance therapy with intramuscular methylcobalamin.
“(A) Tongue of a 69-year-old woman in Japan with pernicious anemia presenting as glossitis (smooth and red dorsum of the tongue, without lingual papillae). (B) One month after starting treatment with methylcobalamin, her tongue appears normal.”
Tongue can be considered as a mirror of oral and/or systemic health. An oral medicine expert can be the first to observe the lingual status, and should be familiar with the different diagnoses of these conditions, e.g., being able to link lingual abnormalities with specific etiologic causes. Recognition of alterations relative to tongue’s morphology, in the presence of a negative anamnesis, should lead to more accurate investigations, in order to ascertain if they are manifestations of an underlying systemic condition.
We agree, and believe the tongue can be a particularly useful tool in diagnosing B12 deficiency. For instance, consider this study that enlisted patients from the Department of Oral Medicine, Peking University School and Hospital of Stomatology:
Vitamin B12 deficiency, which may cause serious neuropsychiatric damage, is common in the elderly. The non-specific clinical features of B12 deficiency and unreliable serum parameters make diagnosis difficult. We aimed to evaluate the value of oral “beefy red” patches as a clinical marker of B12 deficiency.
Of 136 patients, 70 had B12 deficiency. Among these patients, the oral “beefy red” patch was observed in 61, abnormal mean corpuscular volume (MCV) was noted in 30, and serum cobalamin levels <200 and <350 pg/mL were seen in 59 and 67 cases, respectively. The “beefy red” patch demonstrated the highest diagnostic validity and reliability, followed by the serum cobalamin levels and MCV. The combination of “beefy red” patch with cobalamin <350pg/mL exhibited better diagnostic value than the combination of “beefy red” patch with cobalamin <200pg/mL, with accuracy of 0.81 vs 0.74 and reliability of 90.4% vs 86.8%.
Combination of oral “beefy red” patch and serum cobalamin level <350 pg/mL appears to be useful for diagnosis of B12 deficiency.
This study emphasizes the diagnostic significance of tongue conditions in identifying B12 deficiency. This is the first study we’ve encountered that regards the beefy-red tongue as a potentially significant oral clinical marker for B12 deficiency.
In the study, 70 out of 134 patients responded positively to a B12 supplement, and were thus categorized as having B12 deficiency. The most notable clinical feature in this group was the presence of beefy-red patches, found in 61 out of 70 patients. The data indicated that the presence of beefy-red lesions was more accurate than MCV and serological parameters, such as B12 blood levels, for diagnosing B12 deficiency:
According to the findings, you might assume that 87% of B12 deficiency patients would exhibit a beefy-red tongue. However, the study has a major limitation, because its sample consists of patients who reported oral soreness, burning sensations, or recurrent oral ulcers. In other words, the sample is biased towards patients with oral symptoms. This likely resulted in an inflated percentage, as in reality it should be closer to 25%.
To determine conclusively whether the beefy-red tongue is a better clinical marker than serological measurements, we would prefer to see this study replicated with a broader dataset, where patients are not chosen based on the presence of oral symptoms.
Nevertheless, this demonstrates the value of oral mucosal changes as a marker for B12 deficiency, which impairs DNA synthesis. The usefulness of oral signs in diagnosing B12 deficiency can be attributed to the rapid division of oral epithelial cells. Generally, the faster the cell turnover rate, the earlier the effects of B12 deficiency will manifest.
This explains the tight bond of B12 deficiency, pernicious anemia and tongue health.
Dentists Could Play a Major Role
Glossitis and glossodynia are commonly seen by the dental practitioner. The awareness that these symptoms in conjunction with other oral signs indicate pernicious anemia is important for the clinician. Correct diagnosis can be made, and neurological complications avoided. Two case reports are presented and typical oral and systemic features of pernicious anemia are discussed.
The beefy-red tongue is often mistaken for other types of red lesions on the oral mucosa, such as geographic tongue and erythematous candidiasis. In the study we just discussed, two clinicians assessed the oral status. They were trained by the principal investigator to recognize the accurate ‘beefy-red’ tongue, defined by its diffuse and vivid appearance, with linear, band-like, or irregular shapes on any area of the oral mucosa.
Since these oral lesions are often initial symptoms of B12 deficiency, dentists, often the first consulted, are well-positioned to aid in early diagnosis and prevent nerve damage. They should receive training to recognize the appearance of a beefy-red tongue.
This study suggests that such oral signs and symptoms “offer the dentist an opportunity to participate in the diagnosis of this condition”. It reported a case of megaloblastic anemia, a condition characterized by impaired DNA synthesis leading to enlarged red blood cells and epithelial alterations, often caused by folate or B12 deficiency.
The patient in the aforementioned paper was advised to add beef liver into her daily diet, as liver is rich in both B12 and folate. As a result, her oral lesions began to disappear within the first week of treatment. By the end of 14 days, all symptoms were completely gone. This underscores the significance of early diagnosis and the ease of treatment when detected promptly. Dentists could significantly contribute to this.
Here’s another case, this time involving a gastric bypass operation, a procedure known for inducing B12 deficiency by damaging the parietal cells in the gut lining. It resulted in megaloblastic anemia, where oral lesions were the first prominent sign.
In conclusion, the data suggests that early identification of the beefy-red B12 deficiency tongue could aid in diagnosis and help prevent nerve damage. Given that dentists are often the first to examine a patient’s mouth, they can play a significant role, and their findings can complement B12 blood levels or other markers.
We believe that glossitis with linear lesions is an early clinical sign of vitamin B(12) deficiency … Early diagnosis is important because neurologic signs could be irreversible.
Atrophic glossitis is often linked to an underlying nutritional deficiency of iron, folic acid, vitamin B12, riboflavin, or niacin and resolves with correction of the underlying condition.