If recovering from your B12 deficiency feels like a top priority, you’re not alone. Though it’s ‘just’ a vitamin, a lack of B12 can have crippling effects. Symptoms range from chronic fatigue and memory issues to persistent breathlessness and a distinct redness of the tongue. Over time, these can progress to more serious neurological abnormalities.
So, you may be wondering:
After initiating treatment, how long does it take to recover from B12 deficiency?
In their paper, Drs. Robert C. Langan and Andrew J. Goodbred of the St. Luke’s Family Medicine Residency Program in Bethlehem, PA, provide a good overview of B12 deficiency recovery and the expected time it usually takes:
Table 4 lists the usual times until improvement for abnormalities associated with vitamin B12 deficiency. In general, patients with an irreversible cause should be treated indefinitely, whereas those with a reversible cause should be treated until the deficiency is corrected and symptoms resolve.
Of course, the reality of recovering from a B12 deficiency is often more intricate than it appears on paper. Although the above table provides good estimations, various factors can influence the recovery process, making each patient’s journey unique.
First, some background. Vitamin B12 plays a crucial role in various bodily functions, and a deficiency can manifest in numerous ways. Interestingly, it can take years for B12 stores to deplete to a point where a deficiency becomes apparent:
Vitamin B12 deficiency affects multiple systems, and sequelae vary in severity from mild fatigue to severe neurologic impairment. The substantial hepatic storage of vitamin B12 can delay clinical manifestations for up to 10 years after the onset of deficiency. Bone marrow suppression is common and potentially affects all cell lines, with megaloblastic anemia being most common. The resultant abnormal erythropoiesis can trigger other notable abnormal laboratory findings, such as decreased haptoglobin levels, high lactate dehydrogenase levels, and elevated reticulocyte count. Symptoms typically include being easily fatigued with exertion, palpitations, and skin pallor. Skin hyperpigmentation, glossitis, and infertility have also been reported. Neurologic manifestations are caused by progressive demyelination and can include peripheral neuropathy, areflexia, and the loss of proprioception and vibratory sense. Areflexia can be permanent if neuronal death occurs in the posterior and lateral spinal cord tracts. Dementia-like disease, including episodes of psychosis, is possible with more severe and chronic deficiency.
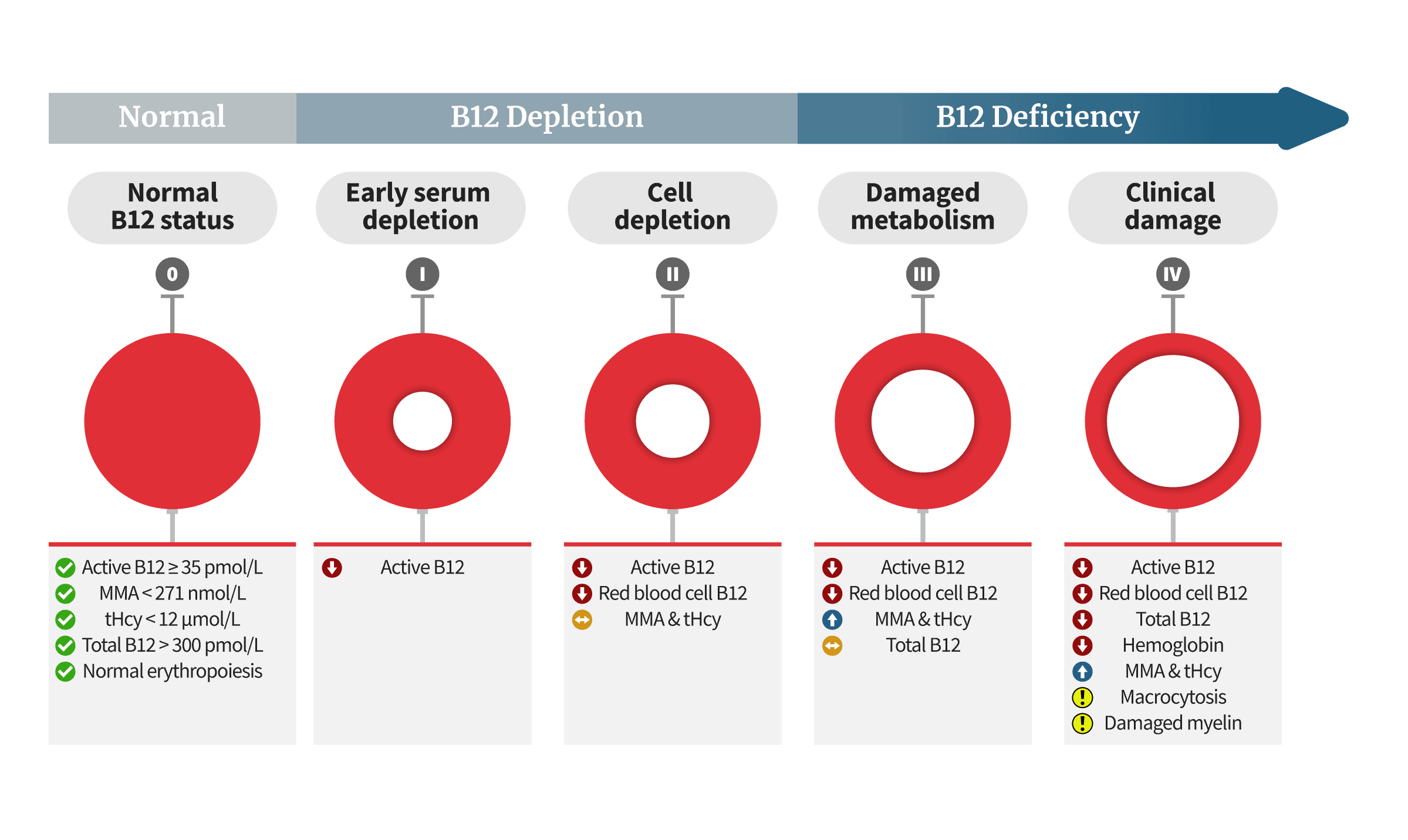
As B12 levels begin to deplete, a deficiency typically progresses through four distinct stages, each characterized by specific biochemical and metabolic changes. These changes, adapted from Dr. Herbert’s model, are outlined as follows:
For us, recovery from B12 deficiency encompasses both the restoration of normal B12 levels (the red circle on the left) and the complete resolution of associated symptoms.
Promptly addressing a vitamin B12 deficiency is imperative to prevent potential irreversible neurological damage. The recovery process, encompassing both symptom alleviation and the replenishment of the body’s B12 reserves, varies in duration and is influenced by several factors. Let’s explore each of them.
Vitamin B12 Deficiency Recovery Time
Here are the factors affecting the time it takes to recover from B12 deficiency:
Severity & Duration: The severity and duration of a B12 deficiency are tightly intertwined, playing a pivotal role in determining the recovery timeline. B12 stores deplete gradually over several years. Once they are significantly diminished, a prolonged deficiency can lead to substantial damage, especially to the nervous system. This extensive damage, in turn, takes longer to completely heal.
Intake: The amount of B12 consumed can affect the speed at which a B12 deficiency is corrected. This is particularly true when the treatment approach involves dietary adjustments, like increasing the intake of B12-rich foods or oral supplements.
Treatment: There are several ways to supplement B12, including tablets, nasal sprays, and injections. However, it’s important to note that not all of these methods are suitable for every patient. In cases where gut absorption issues are present, injections can effectively bypass these problems, potentially leading to a quicker resolution of the deficiency. Conversely, if the deficiency is due to dietary reasons, improvement can occur rapidly once B12 intake is adjusted.
Individual Variability: Factors such as age, overall health, and the presence of other medical conditions can significantly influence an individual’s response to B12 deficiency treatment, as well as the duration of their recovery.
Specific Figures
So, how long does it take to recover from a B12 deficiency in terms of specific numbers? It’s crucial to emphasize that B12 deficiencies are often diagnosed at the fourth stage, when nerve damage may already be present. This complexity makes predicting the exact time-frame for a full recovery challenging—if a full recovery is possible at all.
Nevertheless, there are recognizable patterns to anticipate.
Renowned hematology specialist Professor Ralph Carmel, MD., who has made significant contributions to the scientific understanding of B12 deficiency, states:
Despite an unexplained sense of energy described by some patients in the first 24 hours, hematologic response only begins several days later. The first objective landmark I rely on is the peak reticulocyte count 1 week after starting treatment. Its briskness should be proportional to the severity of the anemia. If reticulocytosis appears blunted, an incorrect diagnosis may be responsible, but I also obtain iron studies because coexisting iron deficiency is frequently obscured before cobalamin is given. The final hematologic landmark is that the blood count, including mean corpuscular volume (MCV), should be completely normal by the eighth week. A failure of homocysteine or MMA to normalize during the first week suggests an incorrect diagnosis, unless renal failure or other causes of metabolite elevation coexist. Cobalamin and holo-transcobalamin II levels are uninformative because they rise with cobalamin influx regardless of therapeutic effectiveness, the extent varying only with the timing in relation to injection.
Neurologic improvement begins within the first week also and is typically complete in 6 weeks to 3 months. Its course is not as predictable as hematologic response, but most studies show little advantage of more intensive cobalamin treatment. Recovery can be slow sometimes, but progression always calls for diagnostic reassessment. Patients with delayed improvement should be offered rehabilitative therapy, particularly for gait, urinary, or bowel dysfunction. Residual disability, estimated to affect 6% of neurologic patients, is the most feared outcome of cobalamin deficiency and is likely to persist if still present after 6 to 12 months of treatment. Irreversibility tends to be associated with more than 6 months of therapeutic delay, but its variability is unexplained.
Both clinical and electrophysiological signs had totally disappeared 3 months later on. This observation demonstrates that, in spite of its poor outcome reported by several authors, peripheral neuropathy induced by vitamin B12 deficiency can recover completely with substitutive treatment.
The rationale behind most symptoms resolving within 3 months is simple:
B12 supplementation results in a swift increase of immature red blood cells within the initial 2-3 days, followed by a gradual normalization of anemia over a 3-month period. Vitamin B12 influences the bone marrow to regulate the formation of red blood cells, which have a life cycle of 90 days. As a result, it takes a full 3 months for all the older, malformed red blood cells to be fully replaced by newly formed, healthy ones.
In other words, your current B12 deficiency symptoms actually reflect your B12 levels from 3 months ago. Therefore, if you began supplementing just 2 months ago, you are still in the process of B12 deficiency recovery, with another month to go.
Throughout this critical three-month recovery period, daily supplementation of B12 is essential. Given that B12 is a water-soluble vitamin, the majority of an injected dose is excreted through urine, leaving only a small fraction for absorption. Regular daily intake ensures a consistent level of B12 in your bloodstream, ready to saturate your cells.
When neurological symptoms are evident, the importance of daily B12 supplementation becomes even more crucial. A lack of daily supplementation could be the reason why B12 injections seem to have little to no effect. Opting for weekly doses significantly slows down the rate of recovery. To effectively go through the B12 deficiency recovery process, it is imperative you commit to daily supplementation for a full 90-day period.
But, how long does it take to recover from B12 deficiency fully? It’s hard to pinpoint the exact number of days, but again, a 90-day period of daily B12 doses should be a default starting point. This time-frame serves as a foundational phase of recovery, and you can assess and adjust your treatment plan based on your progress after these 3 months.
I started one of my patients on liver therapy. This patient, a man in his forties, was critically ill and partially comatose. In spite of his condition, I was able to explain to him that liver might be distinctly useful to him. We found that if a patient were fed half a pound of liver per day, it would take about five days to show an increase in red blood count. But this man seemed more ill on the fifth day. According to the policy laid down, my patient was a candidate for a transfusion. I stayed up very late that night trying to decide to give him the liver. It was a miserable night, but around midnight I noticed that his red blood cell count had increased slightly. That gave me courage to go on with the liver. When I saw his blood count go up, I went home and collapsed into bed, slept very poorly and was back at the hospital at seven o’clock the next morning. I approached his room with fear and trembling, and cautiously peaked around the corner to see if he was still alive. To my great surprise and relief he sat up in bed and cheerfully asked, “What time is breakfast?” His blood count was at the maximum and he not only survived but lived many years.
Several years prior, Murphy, alongside Minot, his fellow Nobel Prize recipient, presented their findings at a conference in Atlantic City. They reported successfully treating 45 patients with significant amounts of raw liver, noting that clinical improvements typically became noticeable after approximately two weeks.
However, it’s important to note that while initial improvements were observed, the complete correction of anemia in these patients, assuming they continued with the raw liver intervention, would have likely taken around 90 days. Again, this is the time required for all the defective red blood cells to be replaced by healthy ones.
The path to recovery hinges on regular, daily supplementation of B12, spanning a minimum of three months to ensure the body has sufficient time to fully heal. Don’t fear high doses; B12 is renowned for its safety, with no established toxicity thresholds even at substantial intake levels. It is considered one of the safest substances to inject.
B12 Deficiency Neurological Symptoms Recovery Time
A patient developed numbness and tingling in distal extremities with subsequent weakness. Evaluation revealed B12 deficiency … Treatment with B12 caused remittance of symptoms and resolution/improvement of abnormalities found on the imaging and electrodiagnostic studies. This case demonstrates that early intervention with B12 supplementation can cause reversal of both central and peripheral nervous system dysfunction.
While red blood cells complete their regeneration cycle every 90 days, fully resolving a vitamin B12 deficiency involves more than just blood cell renewal. Vitamin B12 plays a critical role in maintaining a healthy nervous system, which is particularly vulnerable to the impacts of B12 deficiency. As a result, any nerve damage that has already occurred may require a longer period of time to heal and recover fully.
As emphasized by Professor Carmel, neurological recovery starts within the initial week of initiating treatment, and it generally reaches completion in 1.5 to 3 months. Notably, this time-frame aligns with the 90-day cycle of red blood cell regeneration, suggesting that complete blood cell renewal might often be the limiting factor in recovery, rather than the healing of nerve damage. This alignment reinforces why a period of three months is a reasonable benchmark for assessing recovery from B12 deficiency.
However, recovery from neurological damage can be unpredictable. If symptoms have been present for an extended period before treatment began, there’s a possibility that some of the nerve damage could be irreversible. As Professor Carmel highlights:
Residual disability, estimated to affect 6% of neurologic patients, is the most feared outcome of cobalamin deficiency and is likely to persist if still present after 6 to 12 months of treatment. Irreversibility tends to be associated with more than 6 months of therapeutic delay, but its variability is unexplained.
At this stage, there’s severe damage to the myelin sheath, which is the protective covering of the nerve axons, as well as to the nerve axons themselves. This leads to the degradation of white matter in the spinal cord, resulting in impaired nerve function.
Now, as for the reversibility of nerve damage:
In terms of neurological recovery from B12 deficiency, studies conducted on rats so far indicate that methyl B12 may promote the regeneration of nerves:
Schwann cells (SCs) are constituents of the peripheral nervous system. The differentiation of SCs in injured peripheral nerves is critical for regeneration after injury. Methylcobalamin (MeCbl) is a vitamin B12 analog that is necessary for the maintenance of the peripheral nervous system. In this study, we estimated the effect of MeCbl on SCs. We showed that MeCbl downregulated the activity of Erk1/2 and promoted the expression of the myelin basic protein in SCs. In a dorsal root ganglion neuron-SC coculture system, myelination was promoted by MeCbl. In a focal demyelination rat model, MeCbl promoted remyelination and motor and sensory functional regeneration. MeCbl promoted the in vitro differentiation of SCs and in vivo myelination in a rat demyelination model and may be a novel therapy for several types of nervous disorders.
Human studies are ongoing, and it might take a few more years to derive conclusive evidence applicable to human physiology. However, current knowledge indicates that B12 can decrease the cerebrospinal fluid to serum B12 ratio in men with dementia. Additionally, when combined with B6 and folate, B12 has been shown to enhance blood-brain barrier function in patients experiencing mild cognitive impairment.
None of the patients progressed into dementia during the treatment period. When treated with a vitamin B12-B6-folate combination, patients with mild cognitive impairment and hyperhomocysteinaemia appear to improve their blood-brain barrier function. They may also stabilise their cognitive status. Further investigations are warranted on the role of blood-brain barrier dysfunction in the pathogenesis of dementia.
Based on this, taking prompt action is crucial, especially when B12 deficiency has progressed to the neurological stage, where damage could become irreversible. We recommend initiating a B12 injection therapy, with a preference for methyl B12 injections due to their distinctive nerve-repairing properties. This will not only prevent further deterioration but also potentially aid in the repair of existing damage.
For those without neurological symptoms, the British Society for Haematology suggests administering B12 injections three times a week for a duration of two weeks. In cases where neurological damage is apparent, their recommendation shifts to injections every alternate day for a maximum of three weeks, or until no further progress is noted.
The stakes are too high to take risks by restricting treatment.
After injecting daily for 90 days, you might still experience some neurological symptoms, but your anemia should be resolved. This should alleviate the chronic fatigue and the overall sensation of being unwell, indicating that you are on the path to recovery.
We advise continuing B12 injections beyond the initial three-month period, particularly if any neurological symptoms persist. But even in the absence of neurological symptoms, maintaining this regimen is beneficial, and here’s our reasoning:
Fully Restore Your B12 Reserves
Developing a B12 deficiency often takes about 2-5 years. Therefore, it is unrealistic to expect recovery from such a deficiency to take just a few days.
A B12 deficiency takes years to manifest because the body builds up significant reserves of B12, with the majority being stored in the liver, around 4-5 mg. Only once these stores are depleted will you begin to go through the four agonizing stages of B12 deficiency. Megaloblastic anemia occurs when the reserves drop below 0.1 mg. This is why it takes years before vegans who don’t take B12 supplements start to see symptoms.
Likewise, it takes a long time to replenish these B12 stores. In the U.S., the average daily dietary intake of B12 is a mere 0.0034 mg (3.4 µg), underscoring the need for patience and consistent supplementation. Even with daily injection doses of 1,000 µg, the body absorbs only a fraction of this amount, with the rest being excreted in urine.
Therefore, your objective should extend beyond just alleviating symptoms; it’s crucial to also focus on fully replenishing your B12 reserves. This is the rationale behind our recommendation to continue supplementation well beyond the initial three months. Consider this period as your very vital vitamin B12 recovery time.
B12 Recovery Symptoms
Dr. Joseph Chandy has found that approximately 10% of individuals exhibit B12 deficiency recovery symptoms when they begin supplementation. Surprisingly, some may initially experience a worsening of their condition. This typically happens in the first few weeks following B12 injections but tends to resolve over time.
A number of potential explanations exist for this phenomenon.
In medical practice, treatments that address long-standing damage occasionally appear to exacerbate symptoms initially. A case in point is the Jarisch-Herxheimer reaction in patients undergoing treatment for Lyme disease; this occurs when inflammatory agents flood the system as Lyme bacteria are eradicated. Dr. Chandy posits a similar mechanism at play, suggesting that the swift reparative actions of B12 injections could momentarily overwhelm the body, leading to a temporary intensification of symptoms.
For instance, the exacerbation of symptoms could stem from the nerves readjusting to the changes brought on by B12 supplementation. Alternatively, it might be attributed to a worsening, coexisting illness. It is common for vitamin B12 deficiency to coexist with other medical conditions, as troubles often come in bundles.
If you’re one of the unlucky 1 in 10, don’t panic, and keep supplementing daily for at least three months. You’ll likely feel a lot better. Tolerate the symptoms, and eventually you’ll restore your B12 levels and recover from the B12 deficiency for good.
Prompt Treatment Will Lead to Recovery
It seems that there may be a time-limited window of opportunity for effective intervention in patients with cognitive dysfunction and low serum cobalamin.
Act now, as the window for effective intervention in B12 deficiency is narrow, especially in the presence of neurological symptoms. To prevent nerve damage and expedite recovery, daily injections of vitamin B12 are most effective. However, this raises a critical question: which form of vitamin B12 is most suitable for injection?
Methylcobalamin is the superior choice for B12 injections, effectively increasing cellular B12 levels while simultaneously reducing homocysteine levels, serving a dual purpose. It also provides a valuable methyl donor, aiding in detoxification. Unparalleled in nerve repair, methylcobalamin proves beneficial in treating conditions like peripheral neuropathy, ALS, multiple sclerosis, Alzheimer’s, and Bell’s palsy.
If you can’t find methylcobalamin (edit: we’ve made it available), then the next best alternatives are adenosylcobalamin and hydroxycobalamin, in that order.
We advise against using the cyanocobalamin form of B12. The body must detach its cyanide molecule to utilize it, which depletes your antioxidant glutathione reserves and could potentially elevate homocysteine levels. This process is particularly detrimental for individuals with pernicious anemia or elevated homocysteine.
In terms of dosage, again, the key is often, daily at least (some of our readers inject twice a day). If your doctor is hesitant, then they should at a minimum comply with the NICE guidelines, meaning an injection every two days until there is no further improvement in symptoms. If you don’t want to rely on your doctor, create your own B12 injection kit.
The recovery timeline primarily depends on factors such as the deficiency’s severity and duration, the presence of neurological symptoms, and any absorption issues. Additionally, it depends on whether the treatment effectively targets these concerns. Generally, with daily methyl-B12 injections, most patients can fully recover within 3 months.
However, in cases where nerve damage has been present for an extended period, recovery may take longer than 3 months. The extent of reversibility remains uncertain, but consistent injections of B12 over a minimum of 12 months is recommended to optimize recovery. As Professor Carmel emphasizes:
Neurologic improvement begins within the first week also and is typically complete in 6 weeks to 3 months. … Residual disability, estimated to affect 6% of neurologic patients, is the most feared outcome of cobalamin deficiency and is likely to persist if still present after 6 to 12 months of treatment. Irreversibility tends to be associated with more than 6 months of therapeutic delay …
Continuing daily injections beyond 3 months can potentially aid in further resolving any lingering nerve damage. Additionally, this practice supports your liver in replenishing B12 stores, safeguarding your body against the future re-occurrence of symptoms. It’s crucial to view the restoration of these B12 reserves as a fundamental component in the equation of how much time it takes to recover from B12 deficiency.